Bell’s palsy accounts for 75% of cases but is a diagnosis of exclusion.
Aetiology:
■ Idiopathic facial nerve palsy (IFNP, Bell’s palsy):
1. Commoner in the elderly (>70 years).
2. Spontaneous recovery occurs in 75% of cases.
3. Exposure keratopathy is unusual.
■ Central or peripheral nervous system lesions.
■ Trauma, including iatrogenic causes such as surgery for acoustic neuroma, and facial or parotid surgery.
■ Systemic infections and inflammations.
■ Herpes zoster oticus (Ramsay Hunt syndrome).
■ Middle ear disease.
■ Mastoiditis.
■ Parotid tumours.
Symptoms Related to corneal exposure, failure of the lacrimal pump mechanism, and facial asymmetry.
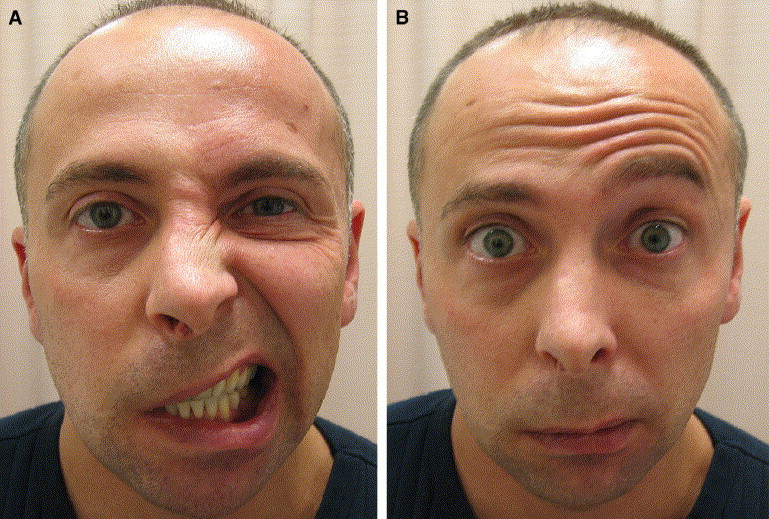
Signs Include facial weakness (including brow ptosis and droop of the angle of the mouth), upper lid retraction, and lower lid atony
History:
Ask about prodromal viral illness, earache, previous facial palsy, trauma, middle ear disease, headache, and dysphonia.
Examination
Examine for underlying causes (see Aetiology above). Regeneration syndromes may be missed. Differentiate between lower and upper motor neurone (central) lesions. Central lesions spare the frontalis action due to bilateral innervation.
Actively exclude vesicles in the external auditory canal (Ramsay Hunt syndrome) because of the risk of CNS complications with immunosuppression. Test corneal sensation and check Bell’s phenomenon and upgaze (the corneal prognosis is guarded if any are abnormal). Examine cranial nerves.
Investigations Consider neuroimaging for patients with:
■ Concomitant focal neurology.
■ Nonresolving facial nerve paresis after 3 months.
Complications
■ Exposure keratopathy and corneal perforation. Contributing factors include upper lid retraction due to unopposed levator activity, lower lid ectropion, lagophthalmos, and failure of tear drainage.
■ Lower lid atony leading to horizontal laxity and ectropion.
■ Aberrant nerve regeneration syndromes including gustatory epiphora, and facial synkineses, e.g. narrowing of the palpebral aperture with lower facial movement.
Treatment

■ Systemic
1. Medical management of IFNP is controversial. Cochrane Database reviews indicate no significant benefit from either systemic steroids (2002) or aciclovir (2001).
■ Ocular
1. Corneal protection
a. Topical lubricants,
b. Botulinum toxin to the upper lid to induce temporary ptosis
c. Temporary tarsorrhaphy with sutures, cyanoacrylate glue, or surgery. A medial (pillar) surgical tarsorrhaphy is preferable to a lateral tarsorrhaphy, because the peripheral visual field is maintained.
d. Lower lid tightening (lateral tarsal strip, which may be ‘augmented’, i.e. placed higher on the orbital rim to aid tear drainage).
e. Lower lid elevation with autogenous fascia lata passed through the length of the lid and sutured medially to the medial canthal tendon, and laterally to the orbital
rim periosteum.
f. Medial (Lee) canthoplasty, medial canthal fixation suture, or medial wedge resection (placing anchoring suture to the periosteum of the posterior lacrimal crest).
g. Upper lid loading with a gold weight (typically for nocturnal lagophthalmos).
h. Upper lid lowering (Müller’s muscle excision for 1–3 mm retraction, or posterior or anterior approach levator recession for larger degrees of retraction).
i. Sural nerve grafting to improve facial tone.
2. Epiphora
a. Residual epiphora is managed once ectropion or lid laxity has been addressed.
b. Gustatory epiphora: botulinum toxin to the lacrimal gland , or direct surgical denervation of the orbital lobe of the lacrimal gland.
c. Dacryocystorhinostomy (DCR) to reduce lacrimal outflow resistance.
d. Lester Jones tube if the patient remains symptomatic at least 9 months following DCR.
3. Aberrent regeneration syndromes
a. These often respond to low-dose botulinum toxin injections.
4. Cosmesis
a. External direct brow pexy (skin and muscle excision with anchoring suture to the periosteum) or endoscopic brow lift (incision above the hair line).
b. Lower lid blepharoplasty if there is tissue laxity and oedema.
c. Angular sling to raise the mouth.
d. Temporalis muscle transfer to create an encircling sling of fascia, passing laterally to medially in both lids.
e. Facial reanimation may be achieved by cross nerve anastomosis.
Follow-up
If there is no recovery of Bell’s palsy within 6 weeks reconsider the diagnosis: 10% of patients with acute facial nerve palsy have a treatable lesion.
Discharge only when all factors contributing to corneal exposure have been addressed and the patient is stable on topical lubricants. This may take months to decades.
